
To mark Melanoma awareness month, The SKINday Times talks to Dermatologist Professor Caitriona Ryan about the steps you can take to protect yourself from skin cancer
Melanoma and keratinocyte skin cancer are two of the most common types of cancers today – but they are also types of the disease where you can take proactive steps to protect yourself as much as possible.
‘Currently there are over 13,000 cases of skin cancer per year in Ireland, about 1300 of which are melanoma. If melanoma is recognised and treated early, approximately 90% are curable, but if it is not, the cancer can advance and spread to other parts of the body, where it becomes difficult to treat and can be fatal,’ warns Professor Caitriona Ryan. Melanoma tends to affect a younger population than most cancers, with major risk factors including white skin, sun sensitivity and family history of melanoma. Sunburn and intermittent sun exposure have also been found to increase the risk of developing melanoma.** ‘Early detection is crucial. The most common forms of non-melanoma skin cancer are basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). If left untreated, some types of non-melanoma skin cancer can spread to other parts of the body but thankfully can almost always be completely cured and treated early.’
Whilst incidence rates are rising worldwide and largely attributed to increasing exposure to ultraviolet (UV) radiation (the main causal risk factor for skin cancer) mortality rates have been stable or have decreased over the past few years – possibly due to increased awareness on the importance of sun protection.*** Being safe in the sun is still the best way to reduce your risk of developing skin cancer, with many steps you can take including wearing a high factor SPF every day (we recommend SPF50), reapplying sunscreen every 2 hours, covering your skin with clothing and wearing a hat and sunglasses. ‘Daily sunscreen use on exposed areas could greatly reduce their risk of skin cancer,’ explains Caitriona. ‘Most Irish people are great at wearing SPF when abroad on holidays but rarely wear it at home, which is where they get most of their cumulative sun damage.’
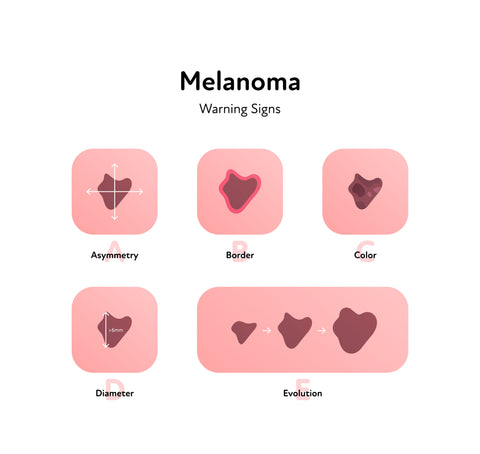
The most important signs to look out for when it comes to melanoma are changes in the size, shape or colour of a mole. Here’s a handy 5-point check, which we call the ABCDE of melanoma:
A is for Asymmetry; Is one half of the spot different to the other half?
B is for Border: Does the spot have an irregular, scalloped, or poorly defined border?
C is for Colour: Does the spot have varying colours from one area to the next, e.g as shades of brown, tan, or black, or areas of red, white or blue.
D is for Diameter: Melanomas tend to be greater than 6 millimetres but they can be smaller.
E is for Evolution: Have you noticed the spot changing shape or appearance?
‘Consult with your GP or dermatologist immediately if you have a changing or new mole, or any skin abnormality, such as a lump, ulcer, lesion or skin discolouration that has not healed after 4 weeks,’ Caitriona advises. ‘While it may not be skin cancer, it's always best to get checked.’ And how often should we examine our skin? ‘Examine yourself from head to toe every month. Learn the moles, freckles and other skin marks that are normal for you. Stand in front of a long mirror and have a hand mirror that you can use to check parts that are hard to see. Ask a relative or friend to check your back or other hard-to-see areas like your scalp or the back of your neck. It may help to take photographs of your skin and compare any changes that occur over time. If you detect something that concerns you, visit your GP.’
Skin cancer: What you need to know
-
Skin cancer occurs when skin cells become abnormal. The most common cancer type in Ireland, 9 out of every 10 skin cancers are caused by UV light radiation from the sun, or from sunbeds.
-
Ultraviolet radiation emitted by the sun is made up of three wavelengths – UVA, UVB and UVC, however, UVC is absorbed by the ozone layer and doesn’t reach the earth’s surface.
-
UVA and UVB rays cause damage to our skin, with exposure leaving us vulnerable to burning, skin ageing and skin cancer.
-
UVB is responsible for most sunburns, but UV damage can start before your skin tans or burns. Excessive short-term exposure causes sunburn, reddening, pain and even blistering and second-degree burns.
-
Factors that influence the intensity of UV radiation from the sun include the position of the sun – the higher the sun is in the sky, the higher the UV level.
Types of skin cancer
Types of skin cancer are divided into two main groups: melanoma and non-melanoma. Melanoma is the least common but most serious form.
Non-melanoma skin cancers (NMSC)
Non-melanoma skin cancers are the result of DNA damage usually due to excess exposure to UV radiation but sometimes also result from exposure to dangerous chemicals. These are the most common types of skin cancer and include basal cell and squamous cell carcinomas, with an estimated average of 12,000 non-melanoma skin cancers diagnosed in Ireland during 2018-2020. In many cases, exposure to the carcinogen has occurred years before the cancer appears.
Melanoma skin cancer
Melanoma is a rarer form of skin cancer, although larger numbers of people are being diagnosed with it each year, with on average 1,100 melanoma skin cancers diagnosed in Ireland during 2018-2020.
Melanoma skin cancer is associated with ultraviolet radiation (UV) exposure from sunbeds, and / or a history of sunburn and commonly begins with a change in a mole or new growth on the skin. Melanoma is an aggressive cancer that develops in the melanocytic cells in the epidermal layer of the skin and can quickly spread to other parts of the body if not detected early. In rarer cases, melanomas can be found in the eye, under the nails or in areas of the body not normally exposed to the sun.
Skin cancer can appear in a number of ways including:
-
A small lump
-
Flat, red spot
-
Firm, red lump
-
A lump or spot that is tender to touch
-
An ulcer that will not heal
-
A lump with a scaly or horny top
-
Rough, scaly patches
-
A new or changing mole
What is the difference between UVA and UVB?
UVA: These rays have a longer wavelength and lower amount of energy than UVB rays. UVA rays account for 95% of the radiation that reaches the earth’s surface and can penetrate the skin deeper than UVB rays, with the ability to enter the dermis - the middle layer of the skin. These rays have skin cancer causing potential and can cause pigmentation and premature ageing.
UVB: These rays have slightly more energy than UVA rays but shorter wavelength, meaning that they only reach the epidermis (the outermost layer of the skin). These types of rays can cause skin burning, as well as also possessing the potential to cause skin cancer. Although they do not penetrate the skin as deeply, the majority of skin cancers are due to UVB.
What does the SPF number mean?
SPF stands for Sun Protection Factor and refers to the sunscreen’s potential to block UVB rays (not UVA). Your sunscreen will display SPF followed by a number ranging from 2 to 50+. This number tells you the time the skin will take to redden with the sunscreen compared to the amount of time it would take to redden without the sunscreen. To break it down, this means if you select and correctly apply SPF 15, it will take your skin 15 times longer to redden as compared to having no sunscreen on at all.
The higher the SPF number, the longer the protection but as SPF is a measure of the degree of protection it gives you from UVB rays, bear in mind that this should not be used to calculate the length of sun exposure.
What about UVA radiation?
If your sunscreen has a UVA seal – a logo with ‘UVA’ inside a circle - this indicates that the product conforms to EU recommendations for UVA protection which is equivalent to at least one third of the SPF. Sometimes, you will see a star rating for UVA. Select one with at least 4 stars for better protection. In the USA and Japan, a PA scale is used to indicate UVA protection, ranging from PA + (Low) to PA ++++ (High).
What are UVA star ratings?
UVA star ratings are often seen across the bottles of many forms of sun protection. Developed in 1992, Boots created this system, which became Europe’s first measurement system for UVA protection. With the rating ranging from 0 to 5, each number indicates the percentage of UVA radiation absorbed by that sun protection, compared to UVB. The higher the star rating, the better the protection against UVA rays. 4 is considered to be the lowest recommended star rating.
Truth V Myths
Sunscreens can harm the ecosystem
New research has suggested that sunscreen can cause harm to the coral ecosystem. The study found that corals absorb oxybenzone from sunscreen and convert it into phototoxins. These molecules then become harmful when exposed to sunlight. The scientists found that coral bleaching events, which can be caused by climate change and warming oceans, make the corals more susceptible to sunscreen accumulation and its damaging effects.* In the new study, environmental chemist Djordje Vuckovic of Stanford University and colleagues found that anemones exposed to fake sunlight while submersed in water containing the chemical died within 17 days.
It’s still unclear what amount of oxybenzone might be toxic to coral reefs in the wild.
Chemicals in sunscreen cause cancer
Cancer.ie revealed that two of their top queries were if chemicals in sunscreens are harmful and if they increase your risk of developing cancer. Current research on the chemicals in sunscreen (oxybenzone, retinyl palmitate and parabens) does not show that they cause cancer and none of these chemicals has been classified as a cancer-causing substance by any major scientific organisations. There have been studies that have suggested that parabens (preservatives used in many cosmetic products, including some sunscreens) act like estrogen in the body, which can speed up the growth of breast cancer tumours but more research is needed to understand this association better.
Only women who sunbathe lots get skin cancer
Skin cancer doesn’t discriminate. In 2013, research showed that almost 6,000 men were diagnosed with skin cancer compared to just under 5,000 women. Skin cancer represents 29% of all cancers in women and 31% of all cancer cases in men, so it’s an issue across genders.

The SKINday Times verdict
Skin Cancer is an insidious disease and so it is important to take precautions when it comes to protecting the skin AND regularly check your skin for any skin changes. We suggest making it a routine and checking the skin weekly whilst applying your body lotion. Encourage the loved ones in your life to do this too. Arranging for a dermatologist to check the skin once per annum may help to map out your skin and help you to recognise any changes also. The regular and consistent application of SPF is crucial. The Irish Cancer Society states that we should be applying a broad-spectrum SPF of at least factor 30 every two hours during the day, and this is necessary every single day, come rain or shine! For the average adult, it is recommended that you need 35mls of sunscreen to cover the whole body. The Irish Cancer Society recommends using a measure of half a teaspoon of sunscreen to cover each arm, the face, neck and ears. Use a measure of one teaspoon for each leg, the front and the back of the body. This is a visible cancer and whilst skin changes can be harmless if you do spot anything unusual, do not delay in getting this assessed by your GP.
Sources
*World Economic Forum, 2022
** Rager EL, Bridgeford EP, Ollila DW. Cutaneous melanoma: update on prevention, screening, diagnosis, and treatment. Am Fam Physician. 2005 Jul 15;72(2):269-76. PMID: 16050450.
*** Leiter U, Keim U, Garbe C. Epidemiology of Skin Cancer: Update 2019. Adv Exp Med Biol. 2020;1268:123-139. doi: 10.1007/978-3-030-46227-7_6. PMID: 32918216.
]]>





















